Chapter 16: Dermal Puncture Equipment and Procedures
MICROSAMPLE CONTAINERS:
Containers come in different sizes to accommodate different volumes of blood. From largest to smallest, they are microcollection tubes, micropipets, and capillary tubes. They are made of plastic and are available with a variety of anticoagulants and additives. The tubes are color coded by additive to match the coding of evacuated containers. Microcollection tubes are used for all types of dermal puncture collections and are the most common type of collection containers used for dermal puncture samples. They are also available with a plastic capillary tube that
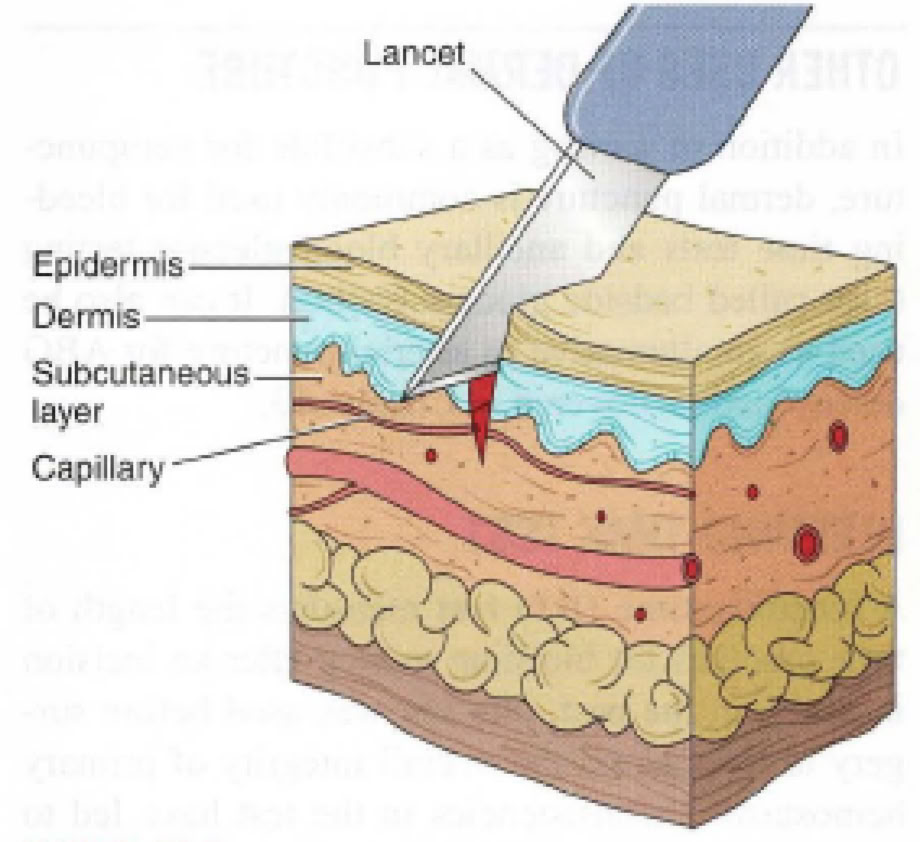
Dermal puncture is an alternative collection procedure when minute amounts of blood are needed for testing, or for patients for whom venipuncture is inadvisable or impossible. It is the usual collection procedure for infants.
In addition, it is the standard procedure for the bleeding time test and blood glucose test. The depth of puncture must be carefully controlled to produce adequate flow while avoiding contact with underlying bone.
REASONS FOR PERFORMING DERMAL PUNCTURE
Although venipuncture is the most common way to obtain a blood sample, at times it is impossible or inadvisable to do so. In these situations, dermal
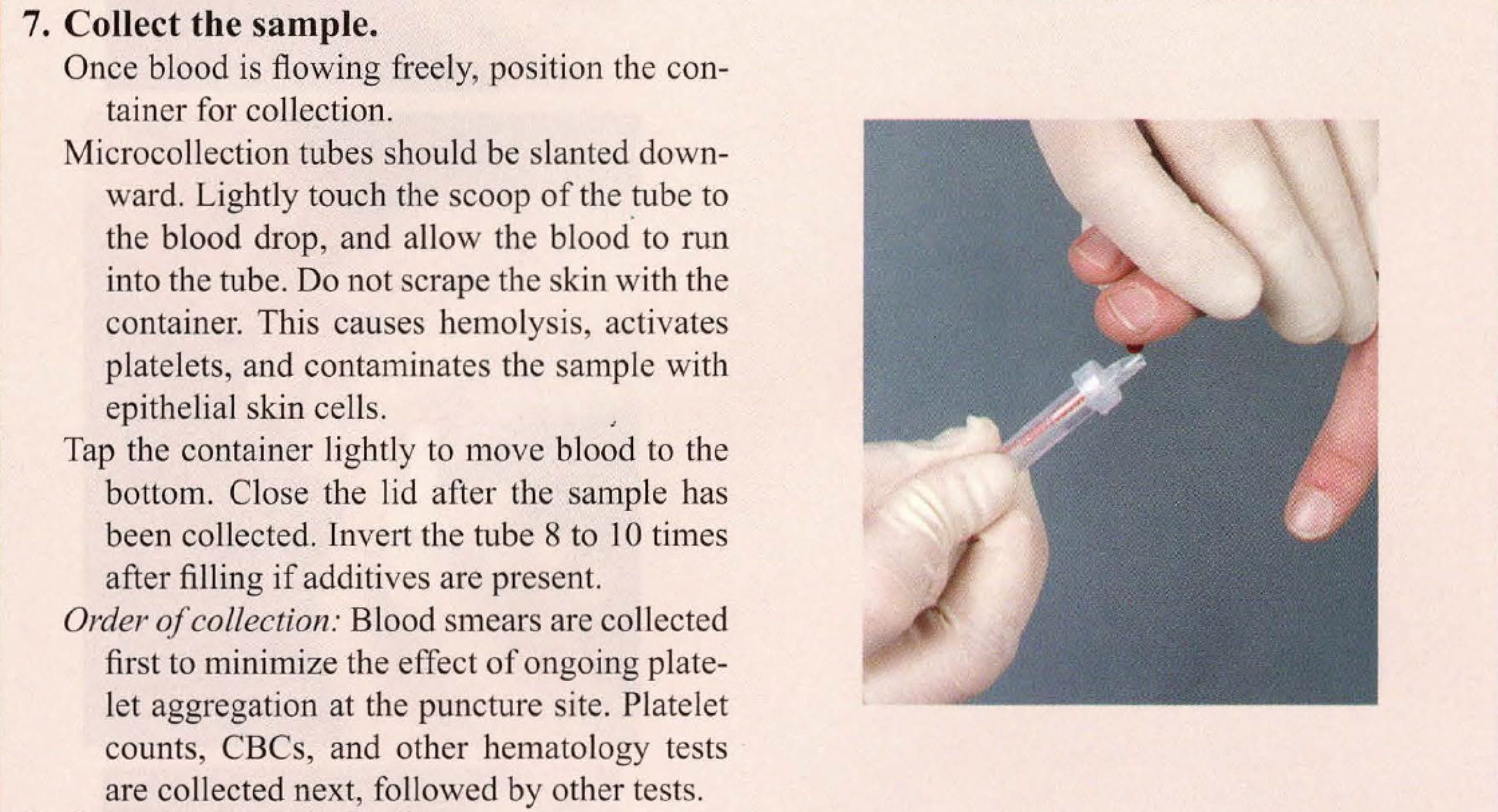
(skin) puncture offers a valuable alternative. Dermal puncture is also used for bleeding time determinations and ancillary blood glucose testing and can be used as an alternative to arterial puncture for arterial blood gas (ABG) determination.
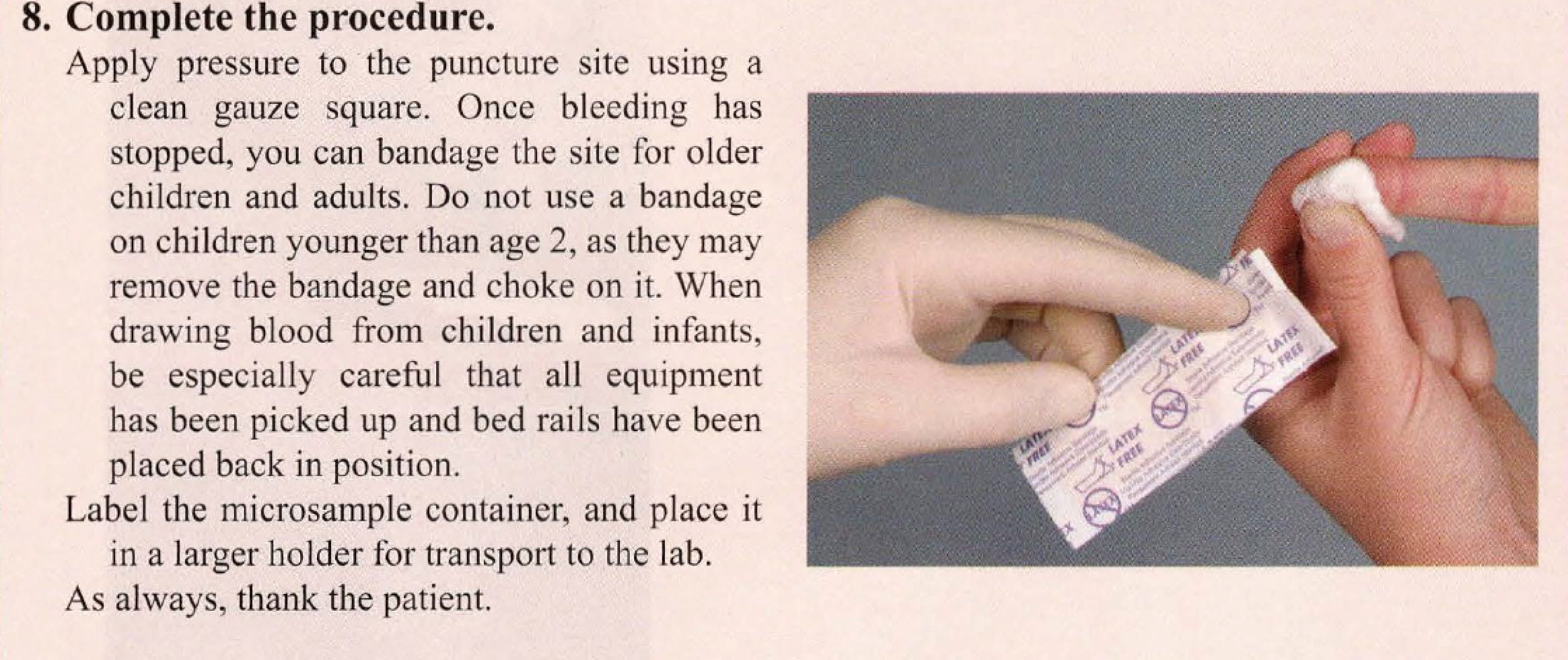
Dermal puncture is preferred in several situations and for several types of patients. Adult patients undergoing frequent glucose monitoring are excellent candidates for dermal puncture, because the test requires only a small amount of blood, which must be taken frequently. Patients requiring frequent blood tests are candidates for dermal puncture. Some patients receiving intravenous (IV) therapy may be dermal puncture candidates.
Dermal puncture is usually the preferred method of collection for newborns, infants, and children younger than 2 years. Young children's smaller veins and lower blood volume make venipuncture both difficult and potentially dangerous. Reducing blood volume through venipuncture is a concern for newborns and infants. It may lead to anemia and even cardiac arrest and death.However, some tests cannot be performed on blood from a dermal puncture. These include blood cultures and most routine coagulation tests.
DIFFERENCES BETWEEN VENOUS AND CAPILLARY BLOOD:
A dermal puncture collects blood from capillaries. Because capillaries are the bridges between arteries and veins, blood collected by , dermal puncture is a mixture of venous blood and arterial blood. The arterial proportion in the sample is increased when the collection site is warmed, as may be done to help increase blood flow before collection. Small amounts of tissue fluid from the puncture site may also be in the sample, especially in the first drop.
EQUIPMENT FOR DERMAL PUNCTURE
Dermal puncture equipment allows the phlebotomist to puncture the skin safely and collect the sample quickly and efficiently, with a minimum of discomfort for the patient.
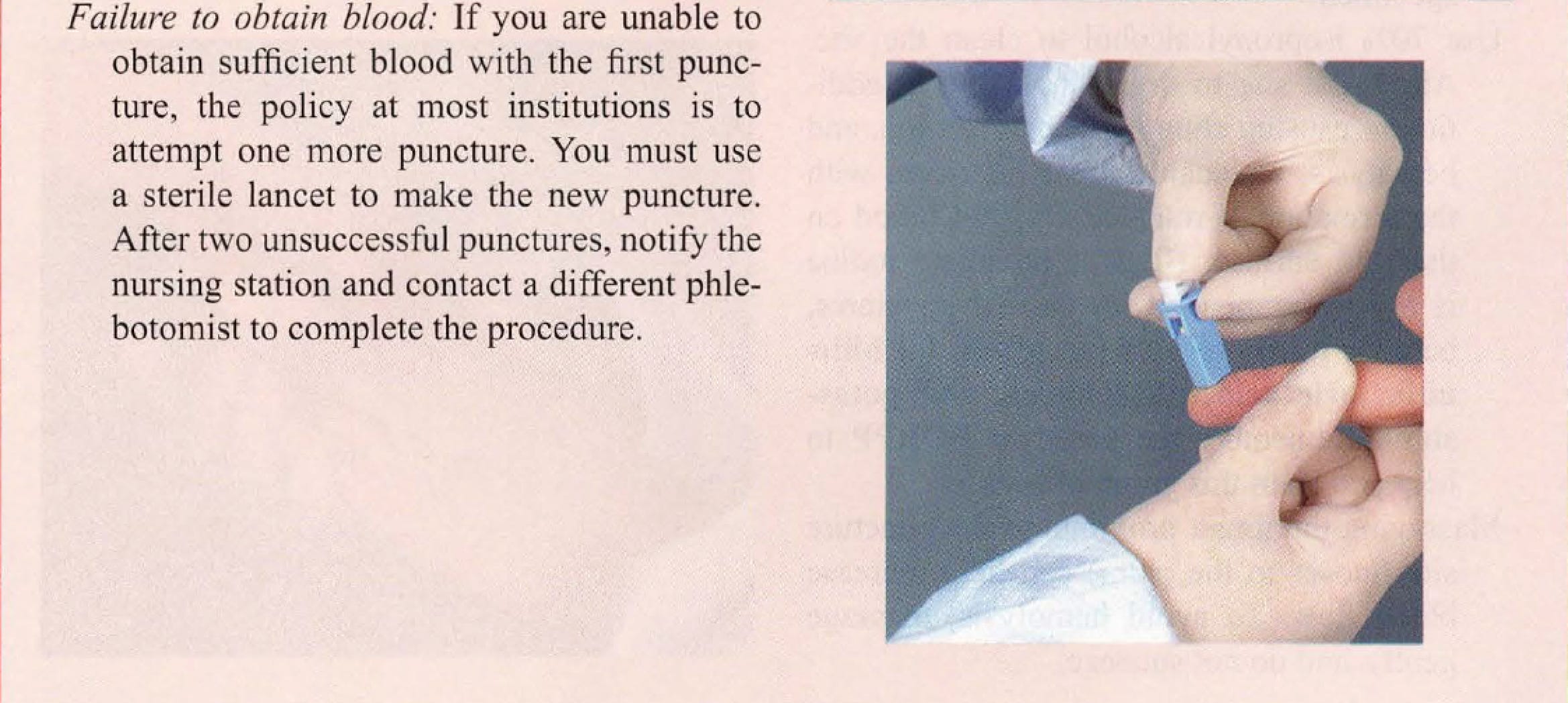
SKIN PUNCTURE DEVICES:
There are many types of skin puncture devices. The oldest and simplest is a handheld lancet, a thin, flat piece of steel with a very sharp tip. These are no
longer used due to Occupational Safety and Health Administration (OSHA) safety regulations that require a retractable blade on the puncture device;
instead, automatic devices have replaced these simple lancets in the modem health care environment.
Automatic puncture devices deliver a swift puncture to a predetermined depth, which can be a significant advantage at sites where the bone is close
to the skin. The dimensions of the puncture are controlled by the width and depth of the point. Devices designed for home glucose testing make a
cut that is too small for multiple tests or for filling several microsample containers and are not used in clinical practice. Safety features include retractable blades and locks that keep a blade from being used
a second time and prevent accidental sticks to the phlebotomist.
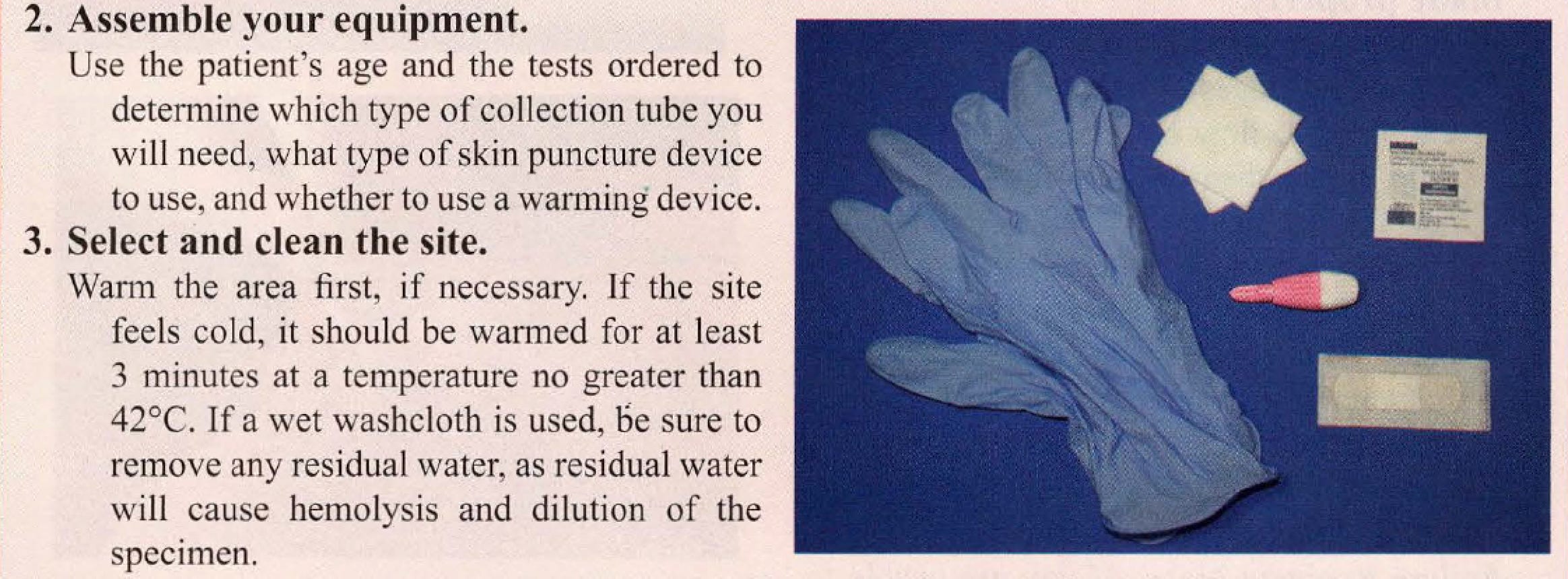
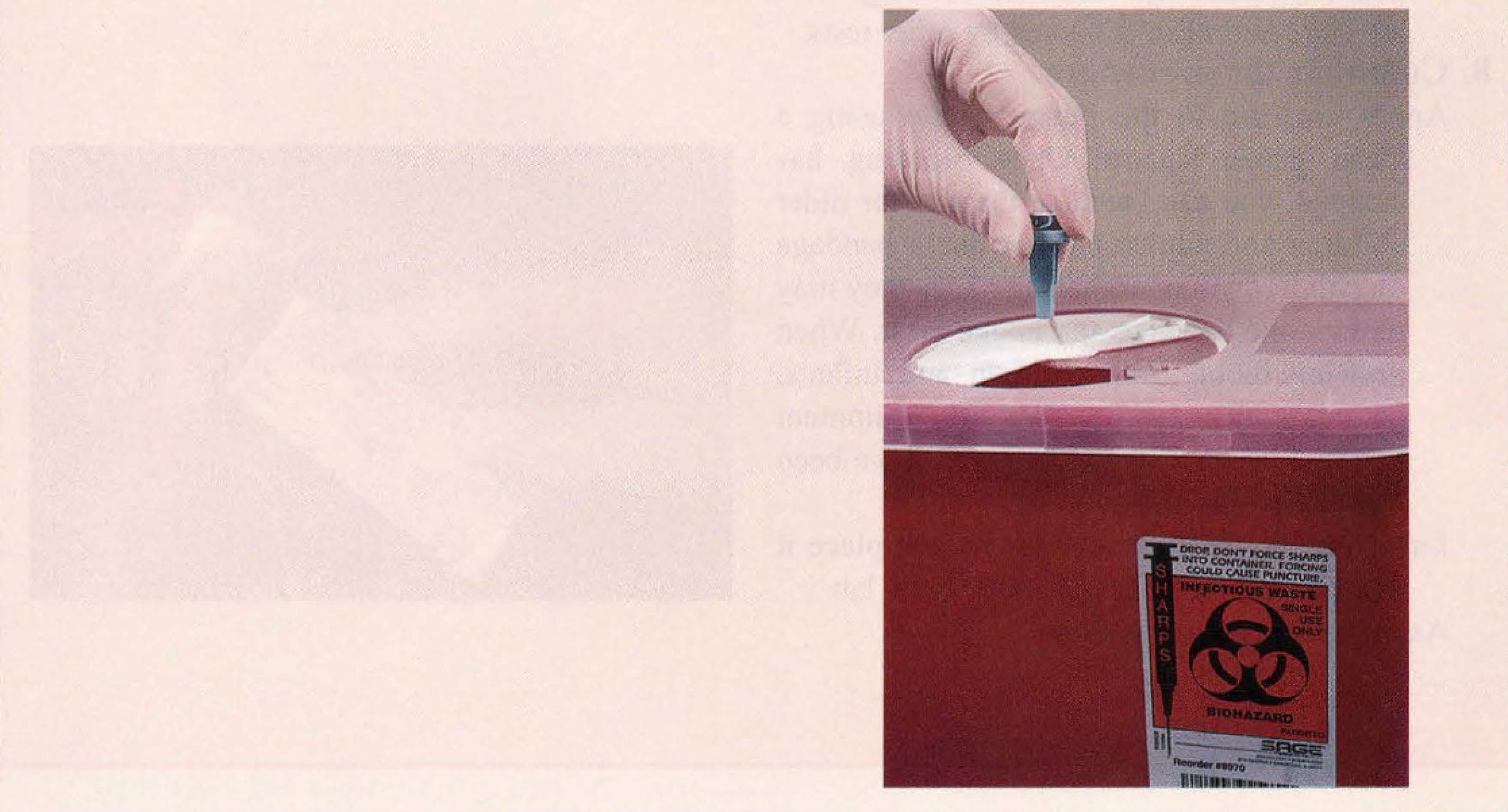
ADDITIONAL SUPPLIES:
As in venipuncture, alcohol pads are used to prepare the site, and gauze pads are used to help stop the bleeding. A sharps disposal container is needed for
the lancet.
Warming devices increase circulation. Simple towels or washcloths may be soaked in warm water and applied to the site. Be sure that the site is completely dry before puncture, however, as residual water will cause hemolysis and dilution of the specimen.
Commercial warming packs are also available. The pack is first wrapped in a dry towel and then activated by squeezing. Such "heel warmers" are often used when blood must be collected from infants. The temperature of the device should not exceed 42°C, and it should be applied for 3 to 5 minutes.
Glass slides are used to prepare blood smears for microscopic examination of blood cells.
SITE SELECTION
GENERAL CONSIDERATIONS:
Dermal puncture should be performed on warm, healthy skin that is free of scars, cuts, bruises, and rashes. The site must be easily accessible and have
good capillary flow near the skin surface, but there must be enough clearance above the underlying bone to prevent the lancet from accidentally contacting it. Bone puncture can lead to osteochondritis, a painful inflammation of the bone or cartilage, or osteomyelitis, a potentially serious, sometimes fatal, bone infection.
You should also avoid skin that has been damaged or compromised in any way. Specific areas to avoid include skin that is callused, scarred, burned, infected, bruised, edematous, or bluish. Also avoid previous puncture sites , and sites where circulation or lymphatic drainage is compromised.
PUNCTURE DEPTH AND WIDTH:
To minimize the risk of inflammation and infection, the lancet should never penetrate more than 3.0mm. For a heel puncture, the maximum depth is
2.0 mm, because the calcaneus, or heel bone, can lie very close to the surface. For premature babies, the recommended depth is 0.65 to 0.85 mm.
Puncture width should not exceed 2.4 mm. At the right site, this achieves adequate blood flow but remains well above the bone.
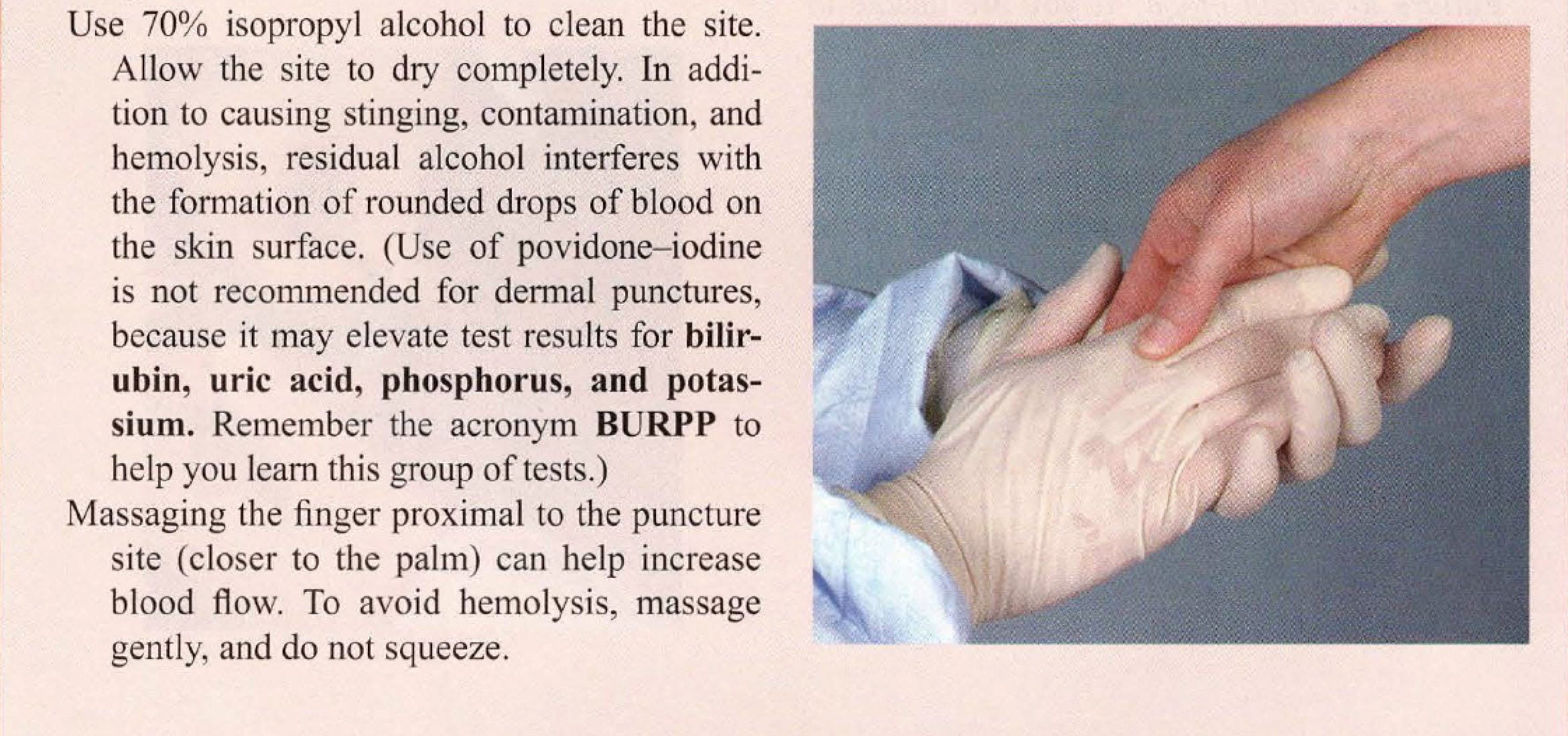
DERMAL PUNCTURE SITES FOR ADULTS AND OLDER CHILDREN:
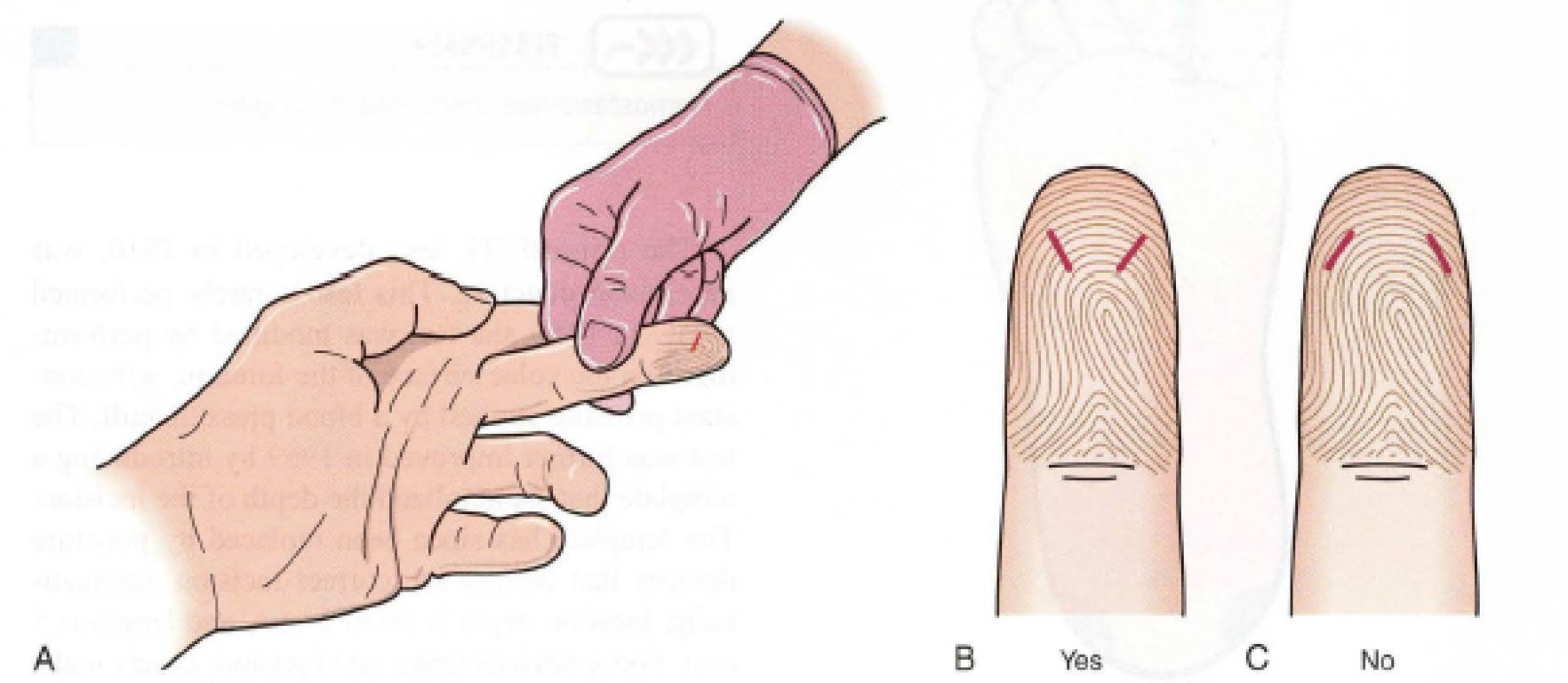
For adults and for children older than 1 year, dermal punctures are almost always performed on the fingertips of the nondominant hand. The best sites are the palmar surface of the distal segments of the third (middle) and fourth (ring) fingers. The thumb is likely to be callused, and the index finger's extra nerve endings make punctures more painful. The puncture should be made near the fleshy center of the chosen finger. Avoid the edge of the finger, as the underlying bone is too close to the surface. The puncture should be made perpendicular to the ridges of the fingerprint, which lessens the flow of blood into the grooves.
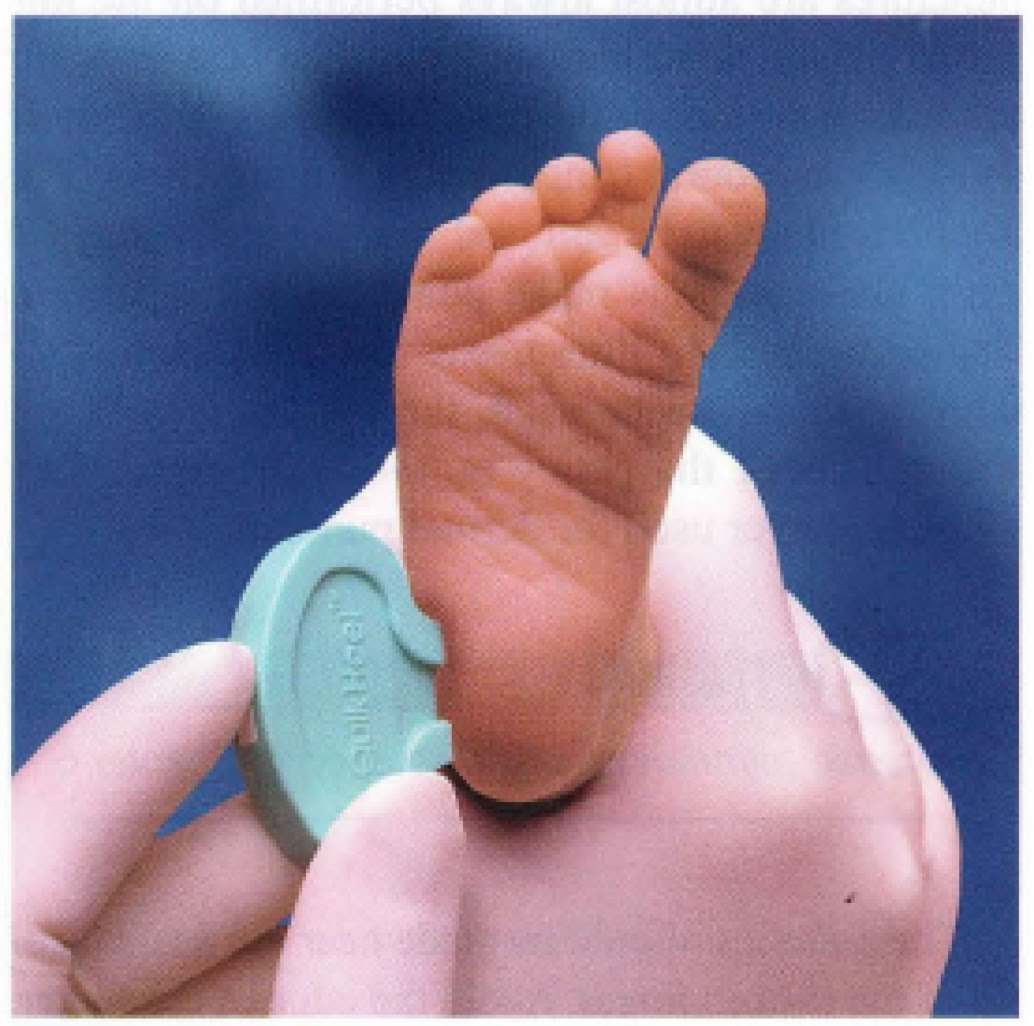
DERMAL PUNCTURE SITES FOR INFANTS:
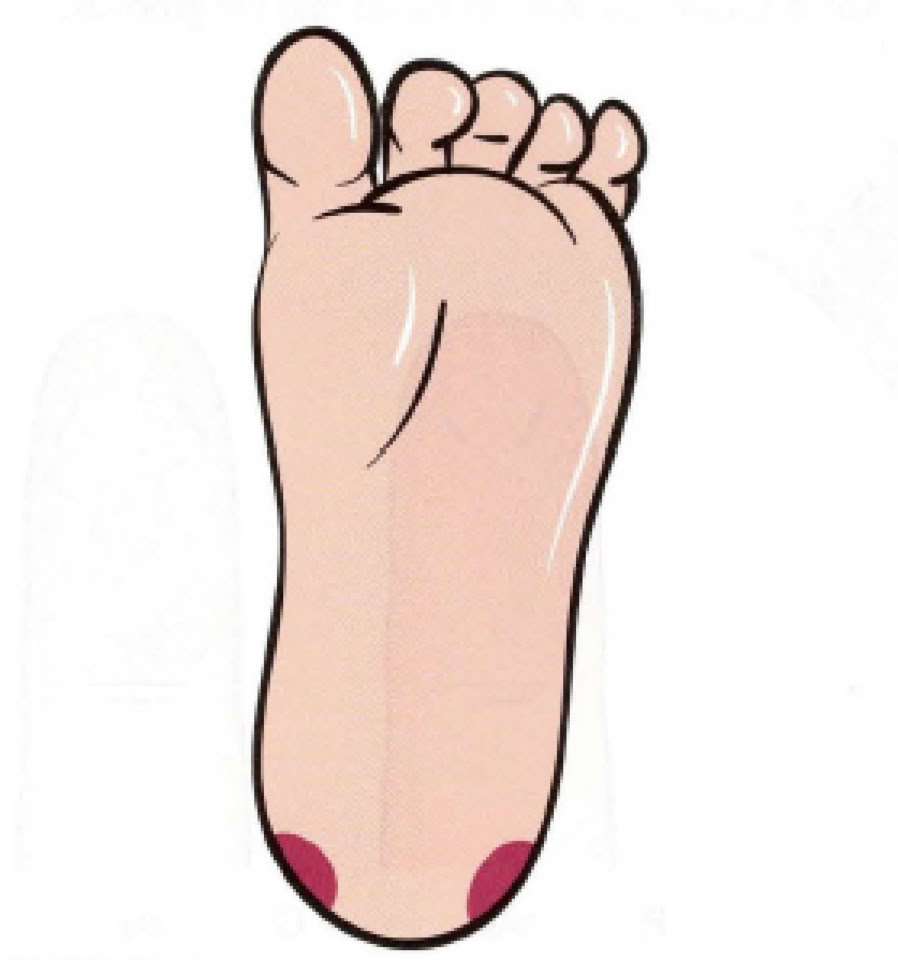
For children younger than I year, there is too little tissue available in any of the fingers. For this reason, dermal puncture is performed in the heel. Only the medial and lateral borders of the plantar (bottom) surface can be used. The center of the plantar surface is too close to the calcaneus, as is the posterior (back) surface. The arch is too close to nerves and tendons. For older infants, the big toe may be used if the heel is unacceptable. Be aware that the heel may be callused on young children who have begun to walk.
BLEEDING TIME TEST
A bleeding time (BT) test measures the length of time required for bleeding to stop after an incision is made. In the past, this test was used before surgery to help assess the overall integrity of primary hemostasis.
The original BT test, developed in 1910, was an earlobe puncture. This test is rarely performed today. In 1941, the test was modified by performing it on the volar surface of the forearm, with constant pressure applied by a blood pressure cuff. The test was further improved in 1969 by introducing a template that standardized the depth of the incision. The template has since been replaced by puncture devices that deliver the correct incision automatically. Incision depth is set at 1 mm, and length is 5 mm. Some devices make one incision; others make two incisions at the same time.